Displasia dell'anca
Disciplinare per il controllo ufficiale della displasia dell'anca e del gomito dei cani iscritti al libro genealogico. D.M. n.11048 del 18.6.2009
ALLEGATO N. 4
Classificazione FCI della displasia dell'anca
Per informazioni sulle centrali di lettura ufficiali italiane:
Ce.Le.Ma.Sche FSA
ALLEGATO N. 4
Classificazione FCI della displasia dell'anca
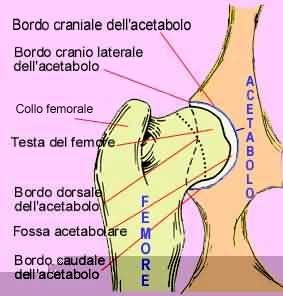
- Grado A: nessun segno di displasia dell'anca (HD 0 / HD -).La testa del femore e l'acetabolo sono congruenti. Il bordo craniolaterale appare netto e leggermente arrotondato. Lo spazio articolare risulta netto ed uniforme.L'angolo acetabolare secondo Norberg è di circa 105° o superiore. Quando inoltre il bordo craniolaterale circonda leggermente la testa del femore in direzione laterocaudale, la conformazione articolare viene definita "eccellente" (A1).
- Grado B: articolazione dell'anca quasi normale (HD 1 / HD +/-).La testa del femore e l'acetabolo appaiono leggermente incongruenti e l'angolo acetabolare secondo Norberg è di circa 105° oppure il centro della testa del femore si trova medialmente al bordo acetabolare dorsale con congruità della testa del femore e dell'acetabolo.
- Grado C: leggera displasia dell'anca (HD 2 / HD +).La testa del femore e l'acetabolo appaiono incongruenti, l'angolo acetabolare secondo Norberg è di circa 100° e/o il bordo cranio laterale risulta appiattito. Possono essere presenti irregolarità o segni minori di modificazioni osteoartrosiche a carico del margine acetabolare craniale, caudale o dorsale o della testa e del collo del femore.
- Grado D: media displasia dell'anca (HD 3 / HD ++).Incongruità evidente tra la testa del femore e l'acetabolo con sublussazione. L'angolo acetabolare secondo Norberg è superiore a 90°. Saranno presenti un appiattimento del bordo craniolaterale e/o segni di osteoartrosi.
- Grado E: grave displasia dell'anca (HD 4 / HD +++).Sono presenti modificazioni marcate di tipo displastico delle anche, come lussazione o sublussazione distinta, un angolo acetabolare secondo Norberg inferiore a 90°, un evidente appiattimento del margine acetabolare craniale e deformazione della testa del femore (a forma di fungo o appiattita) o la presenza di altri segni di osteoartrosi.
Per informazioni sulle centrali di lettura ufficiali italiane:
Ce.Le.Ma.Sche FSA
Classificazione BVA della displasia dell'anca:
BVA (British Veterinary Association, Inghilterra) usa un metodo quantitativo di identificazione della displasia dell'anca: il sistema Willis. La lettura della radiografia con il metodo Willis si avvale della suddivisione del complesso articolare in 9 parametri. Ogni parametro esamina le singole articolazioni (destra e sinistra), assegnando un grado di gravità che va da 0 ad un massimo di 6, ad eccezione del parametro 7 che va da 0 a 5. Un punteggio alto indica un'anca in cattive condizioni e lo 0 è segno di assoluta sanità. Il massimo di gravità totale è di 53 punti per anca. Il risultato relativo alle due anche viene indicato con due numeri separati (es.: hipscore 3/1).
Indicazione dei 9 parametri:
1 - the norberg angle (0-6)
2 - subluxation (0-6)
3 - cranial acetabular edge (0-6)
4 - dorsal acetabular edge (0-6)
5 - cranial effective acetabular rim (0-6)
6 - acetabular fossa (0-6)
7 - caudal acetabular edge (0-5)
8 - femoral head and neck exostosis (0-6)
9 - femoral head recontouring (0-6)
2 esempi della lettura della radiografia dell'anca secondo il sistema Willis (BVA):
1 - the norberg angle (0-6)
2 - subluxation (0-6)
3 - cranial acetabular edge (0-6)
4 - dorsal acetabular edge (0-6)
5 - cranial effective acetabular rim (0-6)
6 - acetabular fossa (0-6)
7 - caudal acetabular edge (0-5)
8 - femoral head and neck exostosis (0-6)
9 - femoral head recontouring (0-6)
2 esempi della lettura della radiografia dell'anca secondo il sistema Willis (BVA):
Classificazione OFA della displasia dell'anca
Excellent: this classification is assigned for superior conformation in comparison to other animals of the same age and breed. There is a deep seated ball (femoral head) which fits tightly into a well-formed socket (acetabulum) with minimal joint space. There is almost complete coverage of the socket over the ball.
Good: slightly less than superior but a well-formed congruent hip joint is visualized. The ball fits well into the socket and good coverage is present.
Fair: Assigned where minor irregularities in the hip joint exist. The hip joint is wider than a good hip phenotype. This is due to the ball slightly slipping out of the socket causing a minor degree of joint incongruency. There may also be slight inward deviation of the weight-bearing surface of the socket (dorsal acetabular rim) causing the socket to appear slightly shallow. This can be a normal finding in some breeds however, such as the Chinese Shar Pei, Chow Chow, and Poodle.
Borderline: there is no clear cut consensus between the radiologists to place the hip into a given category of normal or dysplastic. There is usually more incongruency present than what occurs in the minor amount found in a fair but there are no arthritic changes present that definitively diagnose the hip joint being dysplastic. There also may be a bony projection present on any of the areas of the hip anatomy illustrated above that can not accurately be assessed as being an abnormal arthritic change or as a normal anatomic variant for that individual dog. To increase the accuracy of a correct diagnosis, it is recommended to repeat the radiographs at a later date (usually 6 months). This allows the radiologist to compare the initial film with the most recent film over a given time period and assess for progressive arthritic changes that would be expected if the dog was truly dysplastic. Most dogs with this grade (over 50%) show no change in hip conformation over time and receive a normal hip rating; usually a fair hip phenotype.
Mild Hip Dysplasia: there is significant subluxation present where the ball is partially out of the socket causing an incongruent increased joint space. The socket is usually shallow only partially covering the ball. There are usually no arthritic changes present with this classification and if the dog is young (24 to 30 months of age), there is an option to resubmit an radiograph when the dog is older so it can be reevaluated a second time. Most dogs will remain dysplastic showing progression of the disease with early arthritic changes. Since HD is a chronic, progressive disease, the older the dog, the more accurate the diagnosis of HD (or lack of HD).
Moderate Hip Dysplasia: there is significant subluxation present where the ball is barely seated into a shallow socket causing joint incongruency. There are secondary arthritic bone changes usually along the femoral neck and head (termed remodeling), acetabular rim changes (termed osteophytes or bone spurs) and various degrees of trabecular bone pattern changes called sclerosis. Once arthritis is reported, there is only continued progression of arthritis over time.
Severe Hip Dysplasia: assigned where radiographic evidence of marked dysplasia exists. There is significant subluxation present where the ball is partly or completely out of a shallow socket. Like moderate HD, there are also large amounts of secondary arthritic bone changes along the femoral neck and head, acetabular rim changes and large amounts of abnormal bone pattern changes.